






Up to 30% of people with depression don’t respond to treatment with antidepressants. This may be down to differences in biology between patients and the fact that it often takes a long time to respond to the drugs – with some people giving up after a while. So there is an urgent need to expand the repertoire of drugs available to people with depression.
In recent years, attention has turned to psychedelics such as psilocybin, the active compound in “magic mushrooms”. Despite a number of clinical trials showing that psilocybin can rapidly treat depression, including for cancer-related anxiety and depression, little is known about how psilocybin actually works to relieve depression in the brain.
Now two recent studies, published in The New England Journal of Medicine and Nature Medicine, have shed some light on this mysterious process.
Psilocybin is a hallucinogen that changes the brain’s response to a chemical called serotonin. When broken down by the liver (into “psilocin”), it causes an altered state of consciousness and perception in users.
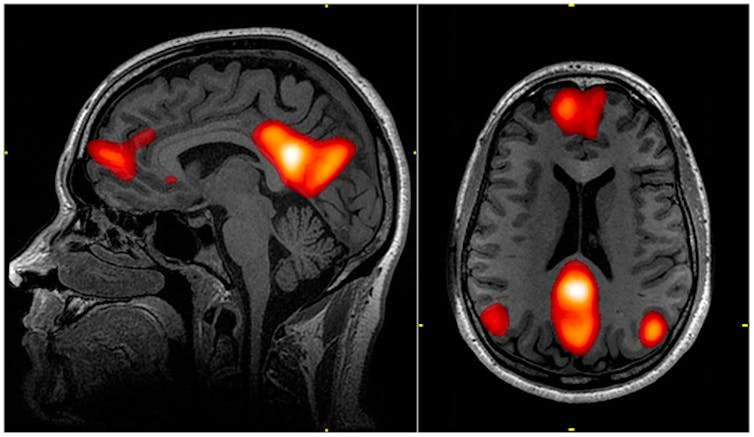
Previous studies, using functional MRI (fMRI) brain scanning, have shown that psilocybin seems to reduce activity in the medial prefrontal cortex, an area of the brain that helps regulate a number of cognitive functions, including attention, inhibitory control, habits and memory. The compound also decreases connections between this area and the posterior cingulate cortex, an area that may play a role in regulating memory and emotions.
An active connection between these two brain areas is normally a feature of the brain’s “default mode network”. This network is active when we rest and focus internally, perhaps reminiscing about the past, envisioning the future or thinking about ourselves or others. By reducing the activity of the network, psilocybin may well be removing the constraints of the internal “self” – with users reporting an “opened mind” with increased perception of the world around them.
Interestingly, rumination, a state of being “stuck” in negative thoughts, particularly about oneself, is a hallmark of depression. And we know that patients with higher levels of negative rumination tend to show increased activity of the default mode network compared with other networks at rest – literally becoming less responsive to the world around them. It remains to be seen, however, if the symptoms of depression cause this altered activity, or if those with a more active default mode network are more prone to depression.
New results
The most compelling evidence of how psilocybin works comes from a double-blind randomised controlled trial (the gold-standard of clinical studies) that compared a group of depressed people taking psilocybin with those taking the existing antidepressant drug escitalopram – something that’s never been done before. The trial was further analysed using fMRI brain scans, and the results were compared with other fMRI findings from another recent clinical trial.
Just one day after the first dose of psilocybin, fMRI measures revealed an overall increase in connectivity between the brain’s various networks, which are typically reduced in those with severe depression. The default mode network was simultaneously reduced, while connectivity between it and other networks was increased – backing up previous, smaller studies.
The dose increased connectivity more in some people than others. But the studies showed that the people who had the biggest boost in connection between networks also had the greatest improvement in their symptoms six months later.
The brains of people taking escitalopram, on the other hand, showed no change in connectivity between the default mode and other brain networks six weeks after treatment started. It is possible that escitalopram may bring about changes at a later time point. But the rapid onset of psilocybin’s antidepressant effect means it may be ideal for people who don’t respond to existing antidepressants.
The study proposes that the observed effect may be due to psilocybin having more concentrated action on receptors in the brain called “serotonergic 5-HT2A receptors” than escitalopram. These receptors are activated by serotonin and are active throughout network brain areas, including the default mode network. We already know that the level of binding by psilocybin to these receptors leads to psychedelic effects. Exactly how their activation leads to changes in network connectivity is still to be explored though.
The end of traditional antidepressants?
This does raise the question of whether altered activity of the brain’s networks is required for treating depression. Many people taking traditional antidepressants still report an improvement in their symptoms without it. In fact, the study showed that, six weeks after commencing treatment, both groups reported improvement in their symptoms.
According to some depression rating scales, however, psilocybin had the greatest effect on overall mental wellbeing. And a greater proportion of patients treated with psilocybin showed a clinical response compared with those treated with escitalopram (70% versus 48%). More patients in the psilocybin group were also still in remission at six weeks (57% versus 28%). The fact that some patients still do not respond to psilocybin, or relapse after treatment, shows just how difficult it can be to treat depression.
What’s more, mental health professionals supported both treatment groups during and after the trial. The success of psilocybin is heavily dependent on the environment in which it is taken. This means it is a bad idea to use it for self-medicating. Also, patients were carefully selected for psilocybin-assisted therapy based on their history to avoid the risk of psychosis and other adverse effects.
Regardless of the caveats, these studies are incredibly promising and move us closer to expanding the available treatment options for patients with depression. What’s more, internalised negative thought processes are not specific to depression. In due course, other disorders, such as addiction or anxiety, may also benefit from psilocybin-assisted therapy.![]()
Clare Tweedy, Teaching Fellow in Neuroscience, University of Leeds
This article is republished from The Conversation under a Creative Commons license. Read the original article.



